- Introduction
- Appearance
- Screening
- Long-term effects
- Predicting Skeletal Maturity
- Bracing
- Surgery
Introduction and Prevalence

Neuromuscular (1)

Neuromuscular (2)

Neuromusular X-Ray
Adolescent Idiopathic scoliosis (AIS) is the most common spine deformity and is defined as a curve of over 10 degrees on x-ray. It affects up to 4% of adolescents in the early stages of puberty and a total prevalence range of 0.4-2.5% in Asia. It can be up to 11 times more common in girls. This comparison with boys increase for more severe curves: 2.7 times for ≥10 o, 4.5 times for ≥20o, 8.1 times for ≥30 o, and 8.4 times for ≥40o. AIS has heritability. Up to 11% of first-degree relatives also have AIS. The condition occurs in otherwise healthy individuals and currently has no recognizable cause. Patients with AIS tend to be taller than those without AIS and have longer arm span and leg length. AIS also correlates with abnormal body composition including a lower body weight and lower body mass index than those without the condition.
Clinical presentation

Truncal Shift

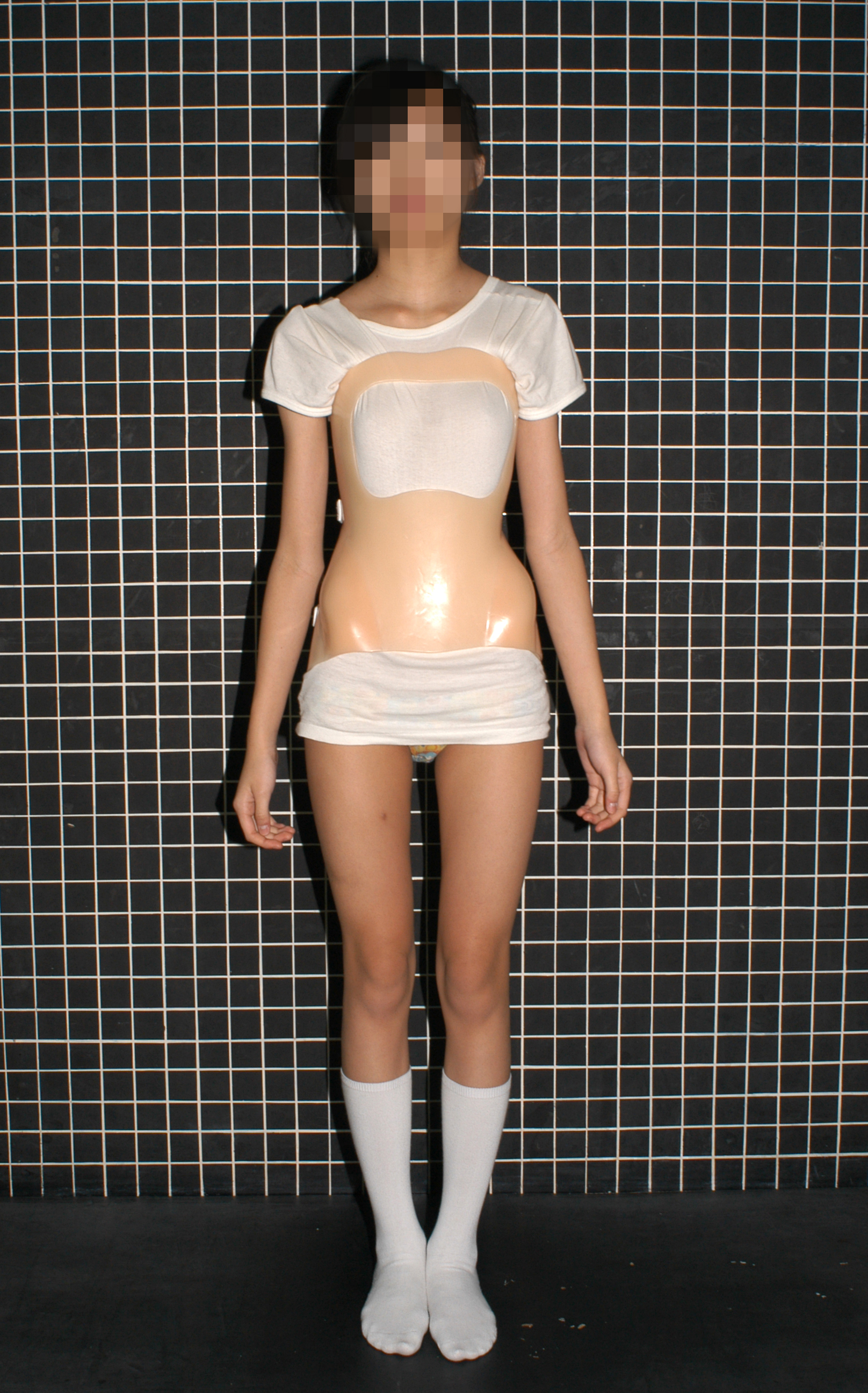
Patient with scoliosis
On clinical examination, patients have shoulder height asymmetry and shift of the trunk. On forward bending, a back ‘hump’ or prominence may occur with rotation of the spine. From the side, patients may have a normal appearance or a hypokyphosis of the thoracic spine. On coronal radiographs, there is a lateral curvature of the spine with a Cobb angle >10o and vertebral rotation. The lateral radiographs may show hypokyphosis. MRI is not routinely performed but should be done if there is suspicion of neurologic abnormality on physical examination, significant back pain or an atypical curve pattern. Atypical curves include short and angular curves, long C-shaped curves, left-sided thoracic curves and right-sided lumbar curves.
Screening in Hong Kong

Forward Bending Test

Scoliometer Measurement
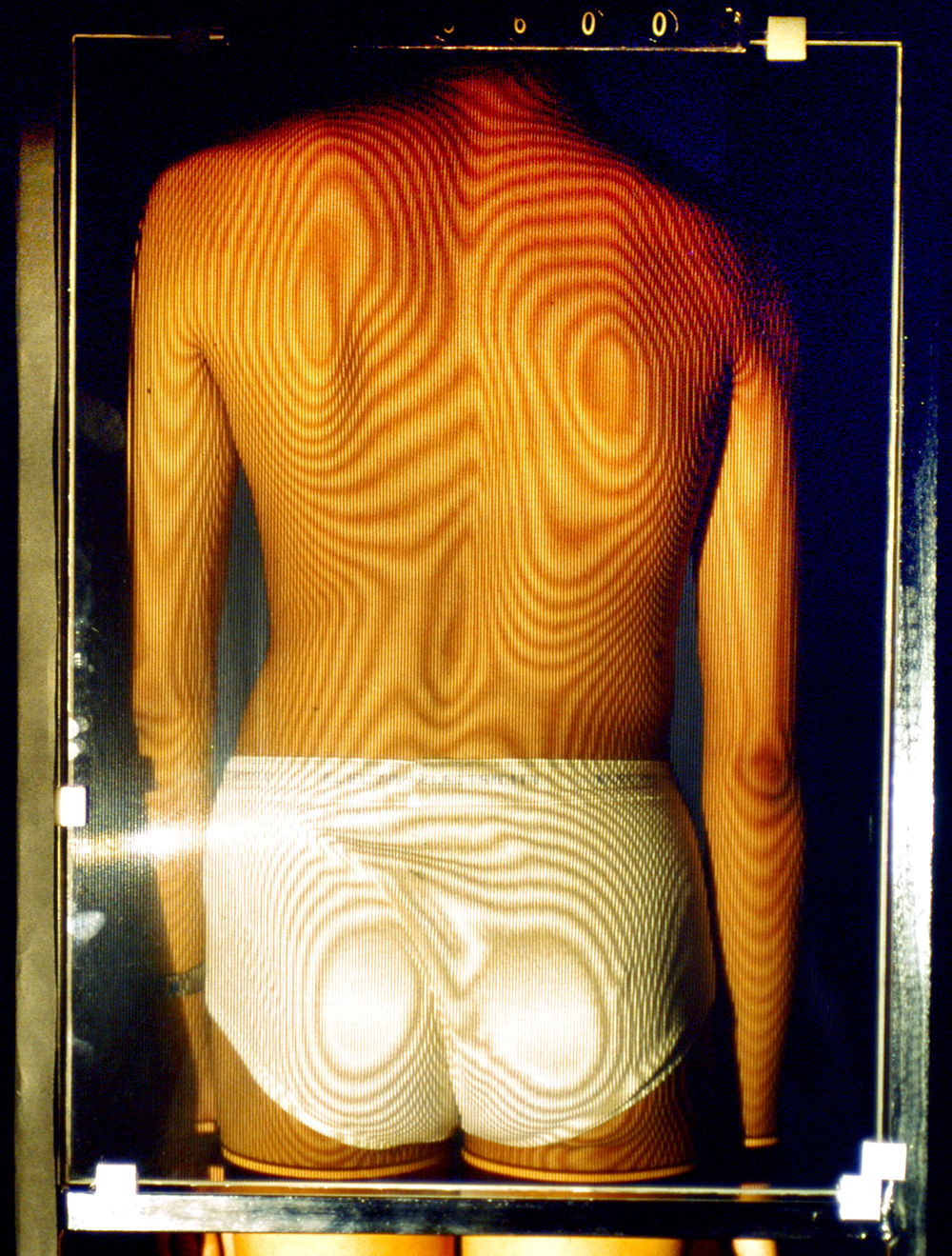
Moiré Topography
Since the early 1995, the scoliosis school screening programme has been initiated in Hong Kong. The purpose of screening is to detect scoliosis at an early stage when it is mild and it can allow early intervention with bracing. Thus, the best time to conduct screening is in the early adolescence since this is when children reach their growth spurt. The commonly used screening tests for AIS are the forward bending test (FBT), the scoliometer measurement of angle of trunk rotation (ATR) and Moiré topography. These are all measures of surface deformity and are safe and easily performed.
Long-term effects of scoliosis
Consequences of untreated scoliosis
AIS occurs in children during their pubertal growth spurt and abnormal skeletal growth is associated with the development and progression of the scoliosis. The risk of progression of deformity is the highest in skeletally immature patients. Thus treatment decisions in AIS are made based on the Cobb angle and risk of progression. With worsening of the spinal deformity, patients may develop future problems such as pain, cardiopulmonary compromise, cosmetic problems and negative psychosocial effects. Lung function is affected by large curve sizes. Some studies showed that Cobb angles of >50° may cause reduced vital capacity and more frequent shortness of breath than smaller curves but this is more significant if the angle reaches 80° or above.
Back pain
Most long-term follow-up of patients with AIS report similar frequency of back pain as those without scoliosis. In the general population, approximately 50% of adults without scoliosis have an episode of lower back pain in any year and 15% may have pain that lasts for more than 2 weeks in any year. However in a 50 year follow-up study conducted in the US, patients with scoliosis had greater frequency, intensity and duration of chronic back pain. But these patients can continue to do work and everyday activities like persons without scoliosis. Most patients with AIS develop early osteoarthritis on x-rays but this may not correlate with back pain.
Pregnancy
No studies have found any correlation between pregnancy and curve progression. Although back pain may occur in up to 35-55% of pregnant women who have AIS, the pain is not disabling and is at the same degree as patients without scoliosis. There are also no increased complication rates or risk of caesarian section.
Predicting Skeletal Maturity
Factors that can predict spinal curve progression include age at diagnosis and maturity factors including spinal curve size and location, age at menarche and the remaining growth. This is decided by many possible grading scales. Our department has developed a unique distal radius and ulna (DRU) classification that determines a child’s remaining growth using a hand radiograph. The degree of closure of the physis of the distal radius and ulna determines the DRU score and the degree of skeletal maturity. This helps doctors decide when to begin and stop bracing and also when surgery is indicated.
Bracing
Boston Bracing (Front)

Boston Bracing (Rear)
Most clinicians agree that if a Cobb angle reaches >20° in a skeletally immature patient, bracing should be initiated. The goal of bracing is to prevent progression of the scoliosis to an angle that requires surgery (Cobb angle of ≥50°) before skeletal maturity. At maturity, the risk of curve progression and risk of surgery decreases. All braces are made of similar thermoplastic material but designs vary. Every brace should aim to restore the normal contours and alignment of the spine by external forces. All braces have similar effectiveness in curve control. Two basic braces are commonly used: Boston or underarm brace which has the brace placed under the axilla and is used in controlling thoracic and lumbar curves. If there is a proximal thoracic curve which usually causes shoulder imbalance, a Milwaukee brace is used which includes a head and neck extension. All braces mainly function during the growth spurt. Some studies show that if patients wore braces >16 hours a day, the success of bracing may reach >90%. Hence, adequate tightness of the brace to exert external forces are important as well as the duration of brace wear.
Physical activities are important complements to brace wear. This improves patient posture and maintains physical health. However, there are no current conclusive evidence that suggests physical activities and scoliosis exercises improve Cobb angles.
Surgery

Patient Pre-op (1)

Patient Post-op (1)
The primary goal of surgery is to prevent scoliosis progression by achieving a spinal fusion of the curves. Surgery is considered for patients with increased risk of curve progression during adult life. This group includes patients with Cobb angles of >40–45°. Fusion in these cases aim to prevent long-term consequences that include reduced pulmonary capacity and disfigurement, reducing the deformity and restoring spinal alignment. The main risks of deformity correction include neurological injury which occurs in approximately 0.05% of surgeries. Early or late infection occurs in approximately 1-2% of cases, implant failure or failure of fusion in approximately 1% of cases, and recurrence or additional deformity in approximately 1%. Long fusions into the lower lumbar spine may also accelerate degeneration.


Patient Pre-op (2)

Patient Post-op (2)
For correction, implants including hooks, wires, cables, and screws are used to hold onto and manipulate the spine via a connection to rods. Fusion of the curve segments require 6-12 months. During this period of time, the implants are necessary to maintain the correction. Once fusion occurs, the correction can be maintained lifelong. The surgery may be performed with an anterior approach (through the chest or abdomen) or through a posterior approach (midline over the spine from the back). With an anterior approach, discectomies or removal of the intervertebral discs can be performed and is a powerful tool for increasing the mobility of the spine and better overall correction of the deformity. Posterior approaches are generally more common as it is a simpler exposure and is extensile (can span the entire length of the spine if necessary).